












































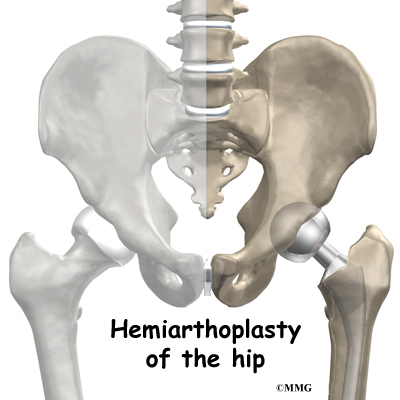
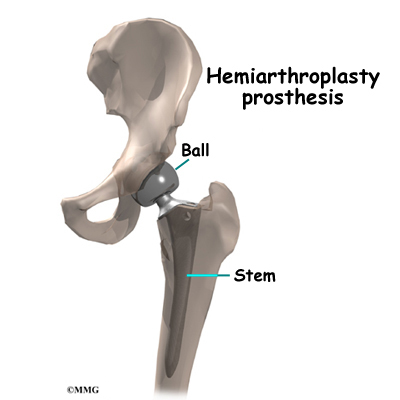
美国某医院 股骨颈骨折病人 Hemiarthroplasty 手术记录

这个帖子发布于 16 年零 286 天前,其中的信息可能已发生改变或有所发展。
88 YO,Female,CHF,HTN
The patient was taken to the operating room and a spinal anesthetic was placed while she was on her bed. After it set up, the patient's feet were wrapped with Webril and Coban and the traction boots for the Hana Orthopedic Table were applied to the feet.
She was then transferred to the operating table and the boots were attached to the traction spars and a perineal post was placed for counter traction. The right hip was then prepped and draped in the usual sterile fashion with time out re-verification being performed.
The area of the planned incision was infiltrated with 0.5% Marcaine with epinephrine and then the incision was made, beginning at 0.1 cm distal, and 2 cm posterior to the right anterosuperior iliac spine and extending distally and slightly posteriorly over the belly of the tensor fascia lata muscle. This was taken down to the subcutaneous tissues and bleeders were electrocoagulated. The fascia overlying the tensor fascia lata muscle was incised and the muscle was teased off the anterior fascial flap. The interval between the tensor fascia lata and rectus femoris was developed. The fascial band was divided. The circumflex vessels were identified and electrocauterized and divided. The fat pad overlying the anterior hip capsule was resected. A capsulotomy was performed beginning at the acetabulum rim and extending along the anterosuperior femoral neck to the intratrochanteric line and then distally.
Cobra retractors were placed intraarticular^ and #1 Tevdek sutures were placed into the capsular flaps thus developed. The femoral neck was divided with a sagittal saw and then a coarse apparatus was used to retrieve the femoral head. It was measured and sized to a 45-mm diameter prosthetic head. The elevating hook for the Hana table was placed around the proximal end of the femur and into the elevation apparatus after which the leg was externally rotated and the hip was placed into extension and adduction, thus presenting the cut end of the femoral neck into the wound.
The neck was exposed with a Mueller retractor as well as a large Homan retractor. Excess tissue from around the anterior, superior, and inferior aspects of the neck was removed. The intramedullary canal was entered by removing the superior neck with a rongeur as well as comminuted neck fragments on a posterior aspect and then opening the canal with a broach. DePuy Summit broaches were then passed up to a size 4 broach and as they were countersunk the calcar rasp was used to remove excess calcar from the femoral neck. A trial reduction with the size 4 Summit stem along with a 45-mm endo head was performed. The fit and fill of the femoral intramedullary canal was acceptable and the leg length showed slight shortening.
It was felt that with some deepening of the position of the stem, in the intramedullary canal, and use of a 0 or +5 Endo head, that leg lengths would be recreated well. Accordingly the hip was redislocated and the stem was sunk deeper into the femoral canal and additional calcar was removed. The stem was then removed and a Summit size #4 cemented stem was selected. A plug was placed into the intramedullary canal and seated at the appropriate depths after which the canal was irrigated with post lavage irrigation system. A double batch of Palacos cement was mixed and then placed into the intramedullary canal and pressurized, after which the #4 cemented stem and centralizer were inserted and seated with removal of excess cement after the cement had hardened, an inspection was made to assure that no excess cement was in place after which another reduction with the standard neck and 45-mm Endo head was performed.
At this time it appeared to be slightly short and therefore it was decided to use a plus 5-mm neck and a 45 mm Endo head. These components were selected, assembled, and placed over the cleansed trunion of the stem, and after thorough irrigation with a post lavage system, a final reduction was performed. Documenting C-arm films were obtained after which the wound was irrigated. A drain was placed into the depths of the wound and exited through a separate stab incision and the capsule was closed utilizing figure-of-8 #1 Vicryl sutures as well as tying of the two #1 Tevdek tag sutures which have been placed into the capsular flaps. The wound was irrigated once again and the fascia overlying the tensor fascia lata muscles was repaired with a running 0 Vicryl suture after which the subcutaneous tissues were closed with interrupted 0 Vicryl and interrupted 2-0 Vicryl sutures.
The skin was closed with skin staples. The drain was connected to a ConstaVac Blood Recovery system and suction was applied. The wound was cleansed, dried and dressed with Xeroform gauze and 4 x 4's followed by a cover roll bandage after which the patient was transferred to the awaiting bed and taken to postanesthesia recovery in satisfactory condition. There were no complications. Sponge, instrument, and needle counts were correct. Blood loss was estimated at 700 cc. The patient received 2 units of packed red cells and 700 cc of lactated Ringers. There were no complications.
有兴趣就翻译一下
The patient was taken to the operating room and a spinal anesthetic was placed while she was on her bed. After it set up, the patient's feet were wrapped with Webril and Coban and the traction boots for the Hana Orthopedic Table were applied to the feet.
She was then transferred to the operating table and the boots were attached to the traction spars and a perineal post was placed for counter traction. The right hip was then prepped and draped in the usual sterile fashion with time out re-verification being performed.
The area of the planned incision was infiltrated with 0.5% Marcaine with epinephrine and then the incision was made, beginning at 0.1 cm distal, and 2 cm posterior to the right anterosuperior iliac spine and extending distally and slightly posteriorly over the belly of the tensor fascia lata muscle. This was taken down to the subcutaneous tissues and bleeders were electrocoagulated. The fascia overlying the tensor fascia lata muscle was incised and the muscle was teased off the anterior fascial flap. The interval between the tensor fascia lata and rectus femoris was developed. The fascial band was divided. The circumflex vessels were identified and electrocauterized and divided. The fat pad overlying the anterior hip capsule was resected. A capsulotomy was performed beginning at the acetabulum rim and extending along the anterosuperior femoral neck to the intratrochanteric line and then distally.
Cobra retractors were placed intraarticular^ and #1 Tevdek sutures were placed into the capsular flaps thus developed. The femoral neck was divided with a sagittal saw and then a coarse apparatus was used to retrieve the femoral head. It was measured and sized to a 45-mm diameter prosthetic head. The elevating hook for the Hana table was placed around the proximal end of the femur and into the elevation apparatus after which the leg was externally rotated and the hip was placed into extension and adduction, thus presenting the cut end of the femoral neck into the wound.
The neck was exposed with a Mueller retractor as well as a large Homan retractor. Excess tissue from around the anterior, superior, and inferior aspects of the neck was removed. The intramedullary canal was entered by removing the superior neck with a rongeur as well as comminuted neck fragments on a posterior aspect and then opening the canal with a broach. DePuy Summit broaches were then passed up to a size 4 broach and as they were countersunk the calcar rasp was used to remove excess calcar from the femoral neck. A trial reduction with the size 4 Summit stem along with a 45-mm endo head was performed. The fit and fill of the femoral intramedullary canal was acceptable and the leg length showed slight shortening.
It was felt that with some deepening of the position of the stem, in the intramedullary canal, and use of a 0 or +5 Endo head, that leg lengths would be recreated well. Accordingly the hip was redislocated and the stem was sunk deeper into the femoral canal and additional calcar was removed. The stem was then removed and a Summit size #4 cemented stem was selected. A plug was placed into the intramedullary canal and seated at the appropriate depths after which the canal was irrigated with post lavage irrigation system. A double batch of Palacos cement was mixed and then placed into the intramedullary canal and pressurized, after which the #4 cemented stem and centralizer were inserted and seated with removal of excess cement after the cement had hardened, an inspection was made to assure that no excess cement was in place after which another reduction with the standard neck and 45-mm Endo head was performed.
At this time it appeared to be slightly short and therefore it was decided to use a plus 5-mm neck and a 45 mm Endo head. These components were selected, assembled, and placed over the cleansed trunion of the stem, and after thorough irrigation with a post lavage system, a final reduction was performed. Documenting C-arm films were obtained after which the wound was irrigated. A drain was placed into the depths of the wound and exited through a separate stab incision and the capsule was closed utilizing figure-of-8 #1 Vicryl sutures as well as tying of the two #1 Tevdek tag sutures which have been placed into the capsular flaps. The wound was irrigated once again and the fascia overlying the tensor fascia lata muscles was repaired with a running 0 Vicryl suture after which the subcutaneous tissues were closed with interrupted 0 Vicryl and interrupted 2-0 Vicryl sutures.
The skin was closed with skin staples. The drain was connected to a ConstaVac Blood Recovery system and suction was applied. The wound was cleansed, dried and dressed with Xeroform gauze and 4 x 4's followed by a cover roll bandage after which the patient was transferred to the awaiting bed and taken to postanesthesia recovery in satisfactory condition. There were no complications. Sponge, instrument, and needle counts were correct. Blood loss was estimated at 700 cc. The patient received 2 units of packed red cells and 700 cc of lactated Ringers. There were no complications.
有兴趣就翻译一下


