












































手术教学录像分享:Quickert术

当退行性下睑内翻合并眼睑水平松弛时,应该同时缩短水平眼睑,这是可以采用Quickert术(横向眼睑切开,外翻缝线+水平眼睑缩短)。 横向眼睑切开阻止了眶隔前轮匝肌的向上移动,外翻缝线缩短了下睑缩肌并将其拉力转移到睑板上缘,而水平眼睑缩短则纠正了眼睑的过度松弛,防止眼睑内翻或外翻。该术式用于“长期”治疗(超过18个月)伴有过度水平眼睑松弛的睑内翻,过度水平眼睑松弛可以通过将眼睑牵拉离开眼球来评估。
The Quickert technique for an entropion remains one of my favorites as it addresses all the factors involved in involutional entropion namely the lid laxity, the overriding and the lacks lower lid retractors. The first step is to mark the incisions.The primary incision goes just below the tarsal, lower lid tassel plate from the punctum to the lateral canthus in a straight line.The degree of lid shortening is dictated by the degree of laxity. And I normally start from a central point and then work out how much tension I want and excise a lateral portion of the lid. The local anesthetic is 2% lidocaine with 1 in 200,000 adrenaline. This can be injected either transconjunctival e or in this instance subcutaneous. The incisions can be made either completely with scissors, completely with blade ,or the mix. I like to use a blade on the skin or indeed cutting coulter on the skin, but then it's very swift to continue with a pair of straight sharp scissors. You need to make sure you've reached fully to the bottom of the tassel plate before making your first horizontal cut. Then swing your arms around, pick up the lid again and make the second horizontal cut. And then finally shortened your lid. In this case, the mark is all but disappeared but I know where I placed it. A little cautery controls the bleeding. And the next step is to take two double armed 6-0 vicryls or 5-0 vicryls and hook the retractors. If you hold on to the conjunctiva, pass the tip of the needle down and see the tip touch onto the conjunctival side but not penetrate, and then lift back up, you can catch hold of the lower lid retractors. This hooking technique is very effective. And then once in place ask the patient to look up, and down, and up and down, and you can check that you have indeed got hold of distractors. The second suture is placed in the same way and I normally find that 2 double armed sutures are plenty. So if you like okay three. But as long as you also address the lower lid laxity, you shouldn't get a recurrence with this technique. Once your lower lid retractors are in place, don't forget to fold the sutures downwards such that when you close the lid margin. they're in place ready to be reattached. The lid margin closure uses the same diagonal tarsal suture, is the primary suture, and this should nibble a first time every time. Lid opposition. And again you carefully reinsert at the exit point from the first lid point lid section. Make sure you have a good bite of tarsal plate. These sutures are buried so is trimmed quite short. And to complete the lid margin closure, the second suture is placed at the bottom edge of the tassel plate and knotted in exactly the same fashion. I usually use 6-0 vicryl throughout the quicker procedure and so far I find this as good as using 5-0 for the retractor sutures. Eyelash suture is then placed or a suture to the lash line. And then another one at the inferior edge of the incised lid margin. To tight things up prior to reattaching the lower lid retractors.The traditional technique for attaching the retractors is to bring them fully out through to the skin below the lashes. But this deep suture coming up to the skin surface, I find, provides the source of irritation, and a risk of infection. I therefore bring each arm up through the orbicularis but stopping short of the skin and then the sutures are tied and buried. I find this gives a faster recovery with less infection and an equally good long-term result in terms of the retractors being advanced . And I found that to 2 double armed sutures perform very well and that a third isn’t necessary. These sutures are then cut nice and short to make them easy to vary. And then I always check that the lower lid retractors are nicely attached by asking the patient to look upwards and downwards, looking for a nice downwards pull on the lid on down gaze. And the final step is similar to close the skin . I carry on with the 6-0 Vicryl. An additional interrupter displaced here for the lid margin. And then , a running stitch goes along the incised inferior skin margin. A significant number of patients in this age group are taking aspirin, often leave them on the aspirin for the surgery, but therefore because there's prolonged use at the end of the surgery, I put chloramphenicol ointment Jelly Net and a pad on and recommend they keep the pad on until the following morning. I normally review the patients at a fortnight, and remove the sutures then. For some patients the sutures can be safely left to dissolve.
以下关于Quickert术式的内容翻译自《A Manual Of Systematic Eyelid Surgery 》第三版,供大家参考
方法
1. 在距离外眦5mm处,从睑缘到睑板下缘,做一个“垂直”切口切开眼睑(图3.7a)。
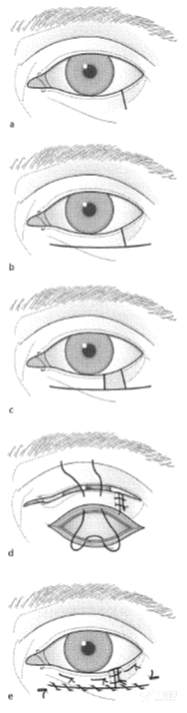
图3.7
2. 在睑板下方做一个水平的全层眼睑切口,直至鼻侧下泪小点。保持剪刀水平在同一水平剪切皮肤和结膜。
3. 在外侧做一个类似的切口,保持水平,不要顺着睑缘的轮廓(图3.7 b)。
4. 识别下眼睑缩肌,从横断下方约2mm处通过下睑缩肌和结膜放置3根4 '0'长效可吸收双臂缝线。
5. 重叠两个眼睑瓣,以评估眼睑需要切除的范围,用来补偿过度的水平松弛。从鼻侧眼睑瓣切除此量(图3.7c)。
注意:如果切除如此数量的组织会导致下泪小点过度移位,应首先折叠内眦韧带以稳定它(见p 63)。然后应重新评估过度的水平松弛并像之前一样切除眼睑。
6. 像正常的眼睑修复术一样缝合眼睑的两个瓣(见p11)。
7. 用4'0'双臂长效可吸收缝线在睑板前面和睑板前肌肉后面穿过,在睫毛线下1-2mm的皮肤出针(图3.7d)。然后继续按照横向眼睑切开+外翻缝线手术的第6步(图3.7 e)进行。
8. 如果水平眼睑横切面以下有多余的皮肤和肌肉,可对皮肤进行修剪,像眼睑成形术那样向外侧牵拉,多余的皮肤行基底向上的外侧三角切除(见图12.7)。
9. 5天后拆除皮肤缝线,但保留睑缘和外翻缝线10天。
并发症
复发通常是由于未能充分缩短下睑缩肌,可以用下睑缩肌折叠术来纠正。


